Plantar Fasciitis in Athletes
Insights From London’s Sports Medicine Specialists (And What I’m Seeing in Clinic)
If you’re a runner or athlete in London dealing with persistent heel pain, there’s a high chance you’ve either had plantar fasciitis before — or you’re perpetually battling it.
Over the years, I’ve looked after a lot of high-level runners and field sport athletes with plantar fasciitis, and for a few of them, I just didn’t have any luck. I would have loved to have experts to collaborate with, in search of the ‘secret sauce’ that fixes this condition miraculously (spoiler alert: doesn’t exist).
Now that I’m working as a sports and spinal physiotherapist in London, I’ve had the opportunity to sit down with some of the city’s leading Foot and Ankle surgeons and Sports & Exercise Medicine doctors — the same clinicians managing professional footballers and elite athletes.
I wanted to understand:
what they think are the leading causes of Plantar Fasciitis
how would they manage this condition
how could Physiotherapists and other health professionals do better to manage this condition?
So instead of giving you another generic “stretch your calves” article, I’m sharing what these conversations revealed — and how we can realistically apply it in our practice.
If you’re an athlete dealing with stubborn heel pain — or a clinician managing plantar fasciitis in a performance population — this is for you.
First: What I’m Actually Seeing in Athletic Plantar Fasciitis
Athletes are WIRED to push, and you have to meet them at their level.
In athletic populations, plantar fasciitis is rarely just “tight calves.”
More often it’s:
A spike in running mileage
Pushing through pain
Not enough rest
Sticking to the running program because of an upcoming event.
Weak foot intrinsics
Insufficient tissue tolerance
And very often…
It’s simply too much, too soon.
🦶 The Surgical Perspective: Mr Ioan Tudur Jones
One of the people I’ve had the privilege of sitting in clinic with here in London is Mr Ioan Tudur Jones — one of the founding members of Fortius Clinic and a world-renowned foot and ankle surgeon.
He works closely with professional footballers and elite athletes, so he’s seeing plantar fascia problems where return to performance really matters.
His thoughts on what the main mechanical cause of plantar fasciitis is?
Poor pronation control
(aka: over-pronation during walking/running/sports).
Excessive pronation can cause (or be caused by) posterior tibialis weakness and plantar fascia elongation. The elongation minimises efficient use of the foot's windlass mechanism because of instability during the propulsive phase of gait.
How does Mr Jones manage Plantar Fasciitis?
Broadly:
Around 80% improve within 3–4 months with
Good physiotherapy (addressing causative factors like load management/foot arch/mobility etc).
± orthotics
± shockwave therapy
The remaining 20%? That’s when you need to dig deeper.
We’d recommend imaging (MRI or Ultrasound at least) to get some clarity on what exactly you’re dealing with. Eg: is there a tear? if so, how big? Or is there something else?
If imaging confirms a tear:
PRP may be considered
consider Short-term boot immobilisation (forced de-load for 2-3 weeks)
And if the above REALLY doesn’t help, when everything has genuinely been optimised — rehab adherence, load management, systemic health — then we consider surgical intervention in the form of a medial gastrocnemius release.
It’s rare he needs to do that, maybe performing 1-2/year!
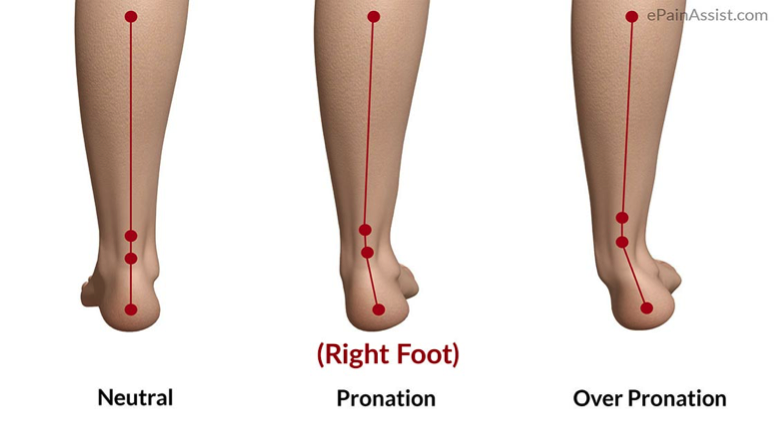
Images depicting what a structural pronated foot looks like in standing.
Just quickly - Windlass mechanism
The windlass mechanism is a complex mechanism in the foot where the plantar fascia (plantar aponeurosis) and intrinsic foot muscles tightens to pull the heel (calcaneus) closer to the Metatarsophalangeal Joint (MTP Joint), creating this nice and high arch (medial longitudal arch). This mechanism happens towards the end of ‘stance phase’, which is when the foot is reaching the end of propulsion and is behind you.
The whole point of this mechanism is to optimise movement efficiency, and reduce how much the muscles have to work to propel you forwards (in simple terms).
Note also that the big toe needs to extend (dorsiflex) to get even more tightening of the plantar fascia for the windlass mechanism to work effectively.
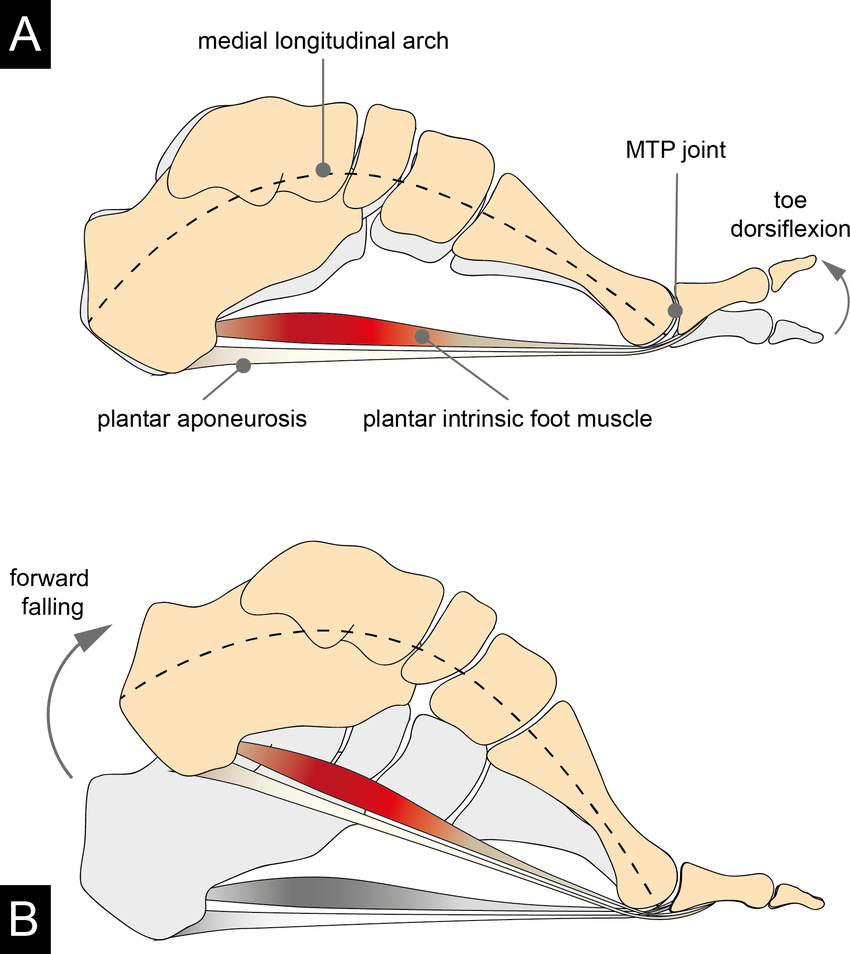
Images depicting the windlass mechanism in action. In image B, the foot is preparing for toe off at the end of stance phase, the big toe is dorsiflexed and the plantar fascia is tight, and the arch is High.
In people with Plantar fasciitis who ‘over pronate’, especially chronic cases, there could be a dysfunction that minimises the use of the windlass mechanism, which then creates excessive pressure through the plantar fascia, potentially leading to the development of Plantar Fasciitis. Over pronation either structurally or functionally, does a few things that hinders this mechanism
Lower Arch! You’ll see this if you have flat feet.
Elongation of the Plantar fascia (because of the flat foot).
Weakness of the Tibialis Posterior. This muscle is designed to create an arch (supinate), or rather, it controls how much your foot pronates while walking/running/sport.
⚽ The Sports & Exercise Medicine Perspective:
Dr Bhavesh Kumar
Dr Bhavesh Kumar is a highly experienced Sports & Exercise Medicine physician. He works with professional athletes — including serving as a doctor to Reading Football Club — and also consults at Fortius Clinic.
He tends to see the cases that haven’t improved. The chronic ones. The frustrating ones. The ones that have “tried everything.”
His first comment to me just hit the spot!
Most people haven’t actually followed the basics properly. Like actually.
If you’re an athlete reading this - I’m sorry if you feel targeted 😂
That includes:
True load management (Physio’s including myself need to be better at enforcing this, and giving clear, structured guidelines as to what you CAN do).
Addressing flat foot mechanics
Improving ankle dorsiflexion
Restoring big toe extension
Building sufficient strength and tissue tolerance
If those pieces aren’t genuinely optimised, escalation is premature.
To add to Mr Jones’ input, here’s what Dr Kumar would do
Recommend seeing a sports podiatrist for insoles — especially in chronic presentations. This relates back to the whole pronation section above.
Arrange imaging to clarify exactly what we’re dealing with
That scan might reveal:
Calcification
A partial tear (and how significant it is)
Or something like Baxter’s nerve involvement
If there is a tear:
PRP can be considered + he also put forward the potential to be in a boot for a period of forced de-loading.
Steroid injections are generally avoided unless pain is severe and function is heavily limited
Dr Kumar’s main takeaway is to absolutely commit to nailing the basics. Be patient with it and most will see positive results in 3-4 months. This is where you need to work with a Physiotherapist who understands the demands of your sport, and is on board with helping you to achieve your ambitious goals!
🩰 The Dance Physio Perspective: Michelle Sim
Michelle is a dance physiotherapist in Australia — and a dancer herself.
She works with a population that arguably places some of the highest repetitive loads through the foot. Chronic plantar fasciitis is something she manages regularly.
Her emphasis?
Foot intrinsics. Remember the windlass mechanism above? Intrinsic foot muscles help control the foot, and contributes to an efficient windlass mechanism in dynamic, athletic movements.
Some of her favourite exercises to do include:
Proper foot doming (without toe gripping)
Big toe lift while keeping the other toes grounded
Progressing into weight-bearing and performance positions
And honestly, I think we under-prescribe this.
I am guilty of this - never been a foot guy, but I have some free foot content below for you showing some exercises Michelle would recommend 🤝
If pronation control is lacking and the intrinsic system isn’t doing its job, the plantar fascia ends up absorbing load it shouldn’t have to.
Her perspective ties in beautifully with the mechanical picture described by Mr Jones and Dr Kumar.
Resisted big toe flexion in standing.
Tibialis posterior activation in standing (foot supination). This basic exercise works on your ability to control foot pronation.
Penguin taps on your toes. This works on increasing load capacity through your feet, with the big toe in dorsiflexion. Progress by loading with dumbbell/barbell.
My Two Non-Negotiables in Plantar Fasciitis Rehab
Across all of these conversations, two themes keep coming back for me.
1️⃣ Load Management
So often, it’s simply:
Too much. Too soon.
Athletes hate hearing this.
But sometimes you have to know when to deload the tissue, and it’s really our job as Physiotherapists to give the guidelines/frameworks that our athletes can work within.
The whole idea is to calm it down enough so that meaningful loading becomes possible again.
If the fascia is constantly flared, it cannot adapt and you’re going round in circles, or even worse, jumping to steroid injections without having properly gone through the basics 🙃
2️⃣ Better Loading (Rebuilding What the Fascia Is Designed to Do)
The plantar fascia is a load-transfer structure.
Its job is to:
Store energy
Transfer force
Contribute to propulsion and the stretch-shortening cycle
If rehab never restores that capacity, you’re only doing half the job.
One tool I like using is the Fasciitis Fighter — performing calf raises with the big toe extended to tension the plantar fascia via the windlass mechanism.
It’s simple.
But it isolates the fascia far better than a standard calf raise.
I’ve also started incorporating heavy isometric loading, borrowing principles from tendinopathy management.
Build confidence there first.
Then gradually increase:
Dorsiflexion demand
Tensile load
Functional loading
Plyometrics
Return to running
Confidence → Capacity → Performance.
The Bigger Picture for Athletes in London
What I find reassuring is that across surgeons, SEM doctors and physiotherapists, there’s strong alignment.
Plantar fasciitis in athletes isn’t about one magic treatment (sorry I wish it was).
When you approach it this way, outcomes become far more predictable.
Assess it thoroughly → Identify contributing factors → Load Management → Rehab / Treat → Integrate back to sport.
🙏 A Thank You
Before I wrap this up, I want to say a genuine thank you to:
Ioan Tudur Jones
Dr Bhavesh Kumar
Michelle Sim (Bentley represent)
For taking the time to share their clinical perspectives.
These are clinicians working at the highest level of sport — managing professional footballers, elite athletes, and highly demanding populations.
📩 Want More Conversations Like This?
If you found this helpful — especially if you're a physio, sports therapist, S&C coach or health professional — I regularly share deeper insights like this through my email list.
Only when there’s something genuinely worth sharing.
If that sounds useful, you can subscribe below.
About the Author
Ryan is an Australian Sports and Spinal physiotherapist based in London and founder of Physiologic.
He specialises in sports and spinal injuries in runners, field sport athletes, and active professionals who value long-term performance — not quick fixes.
Ryan’s approach combines clear diagnosis, intelligent load management, and structured strength-based rehabilitation. He works closely with leading London sports surgeons and Sports & Exercise Medicine doctors to ensure his patients receive coordinated, high-level care — particularly in complex or persistent cases.
Through his writing, Ryan shares clinical insights and real-world frameworks to help both athletes and health professionals think more clearly about injury management and performance.